
Disclaimer: The content contained in this blog is for informational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician, athletic trainer, or other qualified health provider with any questions you may have regarding a medical condition. If you think you may have a medical emergency, call your doctor or 911 immediately.
Injury: Syndesmotic ankle sprain, more commonly known as a high ankle sprain
Epidemiology: Each year 10 million ankle sprains are documented in the United States (Williams & Allen, 2010). In the athletic population, ankle sprains account for 15% - 20% of all athletic injuries each year, one of the most common sports injuries (Williams & Allen, 2010; Swenson, et al., 2013). At the high school level, based on data collected between 2005 and 2011, 3.13 ankle sprains occur per every 10,000 athletic exposures (defined as 1 practice or competition) (Swenson, et al. (2013). Of these injuries, syndesmotic ankle sprains account for 11% to 17% of all ankle injuries (Williams & Allen, 2010). Syndesmotic ankle sprains are most common in football, wrestling, ice hockey, rugby and lacrosse (Williams & Allen, 2010).
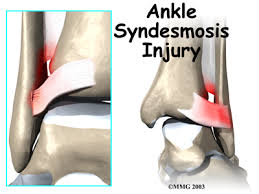
Relevant Anatomy: The distal tibial syndesmosis provides stability to the ankle (talocrural) joint. A disruption of this joint can make it difficult to walk and create sudden changes of direction. The anatomical structures involved in a syndesmotic ankle sprain include:
• Distal tibia
• Distal fibula
• Interosseous membrane
• Anterior inferior tibiofibular ligament
• Posterior inferior tibiofibular ligament
• Transverse tibiofibular ligament
• Interosseous ligament
Mechanism of Injury: Syndesmotic ankle sprains result most often as a result of forced external rotation (twisting foot/leg outward), most often occurring when the foot is planted and lower leg is rotated on the foot. Think of the situation of when an athlete plants his/her foot to change direction and the foot stays planted with the toes pointed out (pigeon toes), but the lower leg rotates internally (rotation of leg toward middle of body).
The injury can also occur when an athlete’s ankle is forced into hyperdorsiflexion. Think about a situation where an athlete is hit or forced into a position where the foot is forced toward the anterior shin (think opposite of pushing gas pedal).
Signs and Symptoms: Most often, athletes who have suffered a syndesmotic ankle sprain will complain of increased pain and instability while pushing off when walking. Tenderness is typically present at the anterior (front) ankle over the distal anterior and posterior (back) inferior tibiofibular ligaments. Depending on the severity of the injury it is likely that the athlete will not be able to bear weight on the injured ankle. While bruising (ecchymosis) and the amount of swelling (edema) varies by injury, a pocket of swelling over the syndesmotic ligaments is most common. In more severe injuries athletes may complain of pain up the distal (lower half) leg or over the deltoid ligament (medial ankle).
Differential Diagnosis: When considering a syndesmotic ankle sprain your healthcare provider will also rule out the following potential injuries:
• Maisonneuve fracture
• Weber fracture
• Deltoid ligament sprain
• Lateral ankle sprain
• Osteochondral lesions and/or bone bruises of talus and distal tibiofibular joint
For athletes who continue to have pain further evaluation may be necessary to rule out:
• Chronic syndesmotic instability
• Syndesmotic scarring
• Impingement because of osteoarthritis (OA)
• Unresolved osteochrondral lesions
Imaging: When being evaluated for a syndesmotic ankle sprain your healthcare provider may request radiographs (X-rays) to rule out potential fracture and to assess the amount of instability (syndesmotic gap). If further evaluation is required an MRI may be requested to evaluate the integrity of the distal tibiofibular ligaments (severity of sprain and which ligaments may be injured).
Management: The management of syndesmotic ankle sprains can vary based on the structures involved and the severity of the injury. Most injuries can be managed conservatively with rest and rehabilitation, but surgery can be an appropriate course of action where there is obvious instability or a fracture requiring stabilization.
Additional Resources:
Rehabilitation of Syndesmotic (High) Ankle Sprains (2010)
Treatment of Acute Ankle Ligament Injuries: A Systematic Review (2013)
NATA Position Statement: Conservative Management and Prevention of Ankle Sprains in Athletes (2013)
Epidemiology of US High School Sports Related Ligamentous Ankle Injuries (2013)
